In a January 8, 2025, article by the Catholic News Agency titled Abortion pills: Where are they legal and illegal?, author Jonah McKeown writes:
“As states continue to legislate on abortion in the post-Roe v. Wade landscape, a major point of contention as a new presidential administration takes office is the two-drug medication abortion regimen, commonly referred to as the abortion pill.
Abortions done via medication, also called chemical abortions, currently account for about half of the abortions that are done in the United States every year. However, many states restrict the use of abortion pills, specifically the first drug in the two-drug regimen, mifepristone. (Emphasis added)”
Take a look at the map below to see where abortion pills are legal, and where they aren’t:
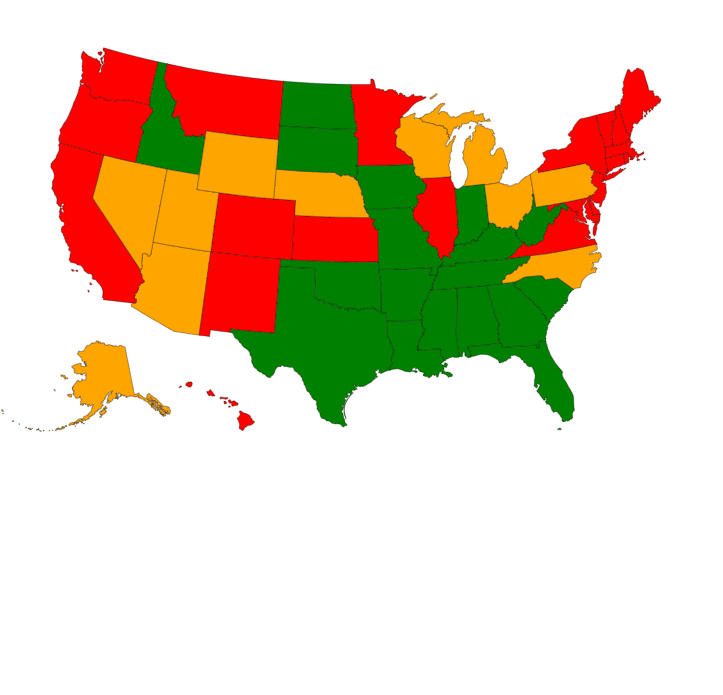
Green is illegal, yellow is limited, and red is legal (go to Abortion pills: Where are they legal and illegal? to click on each state’s specific law)
As the author states:
“At the federal level, mifepristone is approved to abort an unborn child up to 10 weeks’ gestation, having been first approved for such use in 2000.
The drug kills the child by blocking the hormone progesterone, which cuts off the child’s supply of oxygen and nutrients. A second pill, misoprostol, is taken between 24 to 48 hours after mifepristone to induce contractions and expel the child’s body.
Several states, most of which have some pro-life laws in place, have also passed restrictions on abortion pills designed to protect women, including requirements that only physicians may dispense them. These states include Alaska, Arizona, Florida, Georgia, Iowa, Michigan, Nebraska, Nevada, North Carolina, Ohio, Pennsylvania, South Carolina, and Utah. (Emphasis added)”
and
“A large number of states — most of them concentrated in a contiguous cluster in the South and Midwest — ban abortion in most cases but provide exceptions in cases where the life of the mother is at risk or in cases of rape, incest, or fetal anomaly. In these states, access to abortion pills is likely to be very limited or prohibited entirely.
States with total bans on abortion pills include Alabama, Arkansas, Idaho, Indiana, Kentucky, Louisiana, Mississippi, Missouri, North Dakota, Oklahoma, South Dakota, Tennessee, and Texas. “
However, as Mr. McKeown. also writes,
” just because these states have bans on abortion pills in place does not mean the drugs are not accessible; women in those states can still receive them in the mail. Under then-President Donald Trump during the COVID-19 pandemic in 2020, the FDA was given the ability to distribute the drug via mail. The administration of President Joe Biden eventually solidified the practice as a norm in 2023. (Emphasis added)
A group of state attorneys general, led by Missouri, is currently suing the Food and Drug Administration (FDA) over its deregulation of the drug, arguing that abortion drugs have been “flooding states like Missouri and Idaho [where abortion is otherwise regulated] and sending women in these states to the emergency room.”
In addition, Texas Attorney General Ken Paxton recently filed a lawsuit against an abortionist in New York, alleging that she illegally provided abortion drugs to a woman in Texas, which killed the unborn child and caused serious health complications for the mother.”
Sadly, as Mr. McKeown writes:
President-elect Trump has committed to keeping abortion pills accessible during his second term — a major disappointment for pro-life advocates, who have urged Trump to use the FDA’s power to enforce a Comstock Act prohibition on the delivery of “obscene” and “vile” products through the mail, which includes the delivery of anything designed to produce an abortion.”
CONCLUSION
As I wrote in my June 16, 2024 blog “The Supreme Court Rejects Challenge by Pro-life Doctors on Abortion Pill“:
“As Life News reported on June 13, 2024:
“The Supreme Court on Thursday rejected a challenge to the abortion pill mifepristone, meaning the abortion drug will be widely available to continue killing babies and injuring doctors nationwide.
The 9-0 decision says the pro-life doctors who brought the case do not have standing – they were not injured, and so the court does not intervene. That’s even though they sued on behalf of women who were injured by the abortion drug by the thousands – including women who have been killed.” (Emphasis added)”
I have a personal interest in this because I had an unwed daughter who became pregnant and started bleeding without telling me because of embarrassment.
She went to a local ER, where the doctors said she was just having a miscarriage and sent her home.
When the pain and bleeding increased, she called me. I took her back to the ER to demand an ultrasound.
As I suspected as a nurse, her pregnancy was ectopic and emergency surgery was performed.
Afterward, the surgeon showed me the picture he had taken (unasked) during the surgery to remove the then-deceased first-trimester baby, my grandchild. The picture was personally so sad to see but I was comforted that the surgeon cared enough to take a picture of this tiny person and show respect.
We need more respect and help for women with an unexpected pregnancy and their babies than a pill without medical safeguards!”
Related
“Safer Than Tylenol” is Deliberate Medical Abortion Disinformation February 26, 2023


You must be logged in to post a comment.